65 yrs old female with B/L pedal edema, facial puffiness, fever,SOB
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
 DIAGNOSIS
DIAGNOSIS
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
Pt came with c/o of
Pedal edema -10days
Facial puffiness -10days
Fever -7days
Sob -4 days
Dry cough -4 days
HOPI
Pt was apparently asymptomatic 15 days back then she had pedal edema, facial puffiness since 10 days which are not associated with burning micturition,no decreased urine output,no loin pain
C/0 fever since 4 days which is continuous and no diurnal variation,but it is associated with chills and rigors
C/0 dry cough since 4 days,it is associated with pain while coughing
Shortness of breath since 4 days (grade 3-4)
orthopnea+
No PND,chest pain
Past History:
Pt had similar complaints of pedal edema 4 months back which were releived with out any medication
K/c/o DM 2 -30yrs
(Using T metformin-500mg po/od)
N/k/c/o hypertension,TB, epilepsy,CAD,Asthma
Personal history:
Mixed diet
Appetite is decreased
Bowel and bladder - normal
Sleep is adequate.
occasional toddy drinker (last drank 4 months back)
No known allergies.
Family history:
No similar complaints.
General Examination:
Pt is moderately built, moderately nourshised
Pt is c/c/c well oriented to time,place, person
Vitals
No Pallor, Icterus, Cyanosis, Clubbing, generalized lymphadenopathy,
B/l pedal Edema (pitting type)
Vitals:
Temp.- 98F
BP- 110/70 mmHg
PR- 92 bpm
RR- 30cpm
Systemic Examination
CVS
Cardiac sounds :- S1 & S2 - Present
Cardiac murmurs :- NO
RESP. SYSTEM
Dyspnoea :Yes
Wheeze :Expiratory wheeze presenting in all areas.
Position of Trachea : Central
Breadth Sounds : Vesicular
ABDOMEN
Shape of abdomen : Distended
Tenderness : NO
Palpable Mass : NO
Liver : Not Palpable
Bowel sounds: Yes
C.N.S
Level of consciousness : Consciousness: Conscious / Alert
Speech : Normal
Signs of Meningeal irritation a)Neck stuffiness: NO b)Kernig's sign: NO
Cranial nerves- Normal
Motor system - Normal
Sensory nerves- Normal
Glasgow Scale - 15/15
Ultrasound of thorax and abdomen
Impression:-
B/L pleural effusion
Right:- moderate
Left :- mild
Conclusion:- 2DECHO
Moderate TR with PAH , Mild AR , Trivial MR
No RWMA, NO AS/MS , Sclerotic AV
Fair LV function
Diastolic dysfunction
No LV clot
FUNDUS EXAMINATION:
RE:TRACTIONAL RETINAL DETACHMENT ON B SCAN
LE:SEVERE NPDR CHANGES NOTED[TORTUS ,ATTENUATED COTTON WOOLSPOTS+,DOT
HEMORRHAGE SUPERIOR TO DISC+,FIBROUS BANDS EXTENDING FROM DISC]
DIAGNOSTIC PLEURAL TAP:
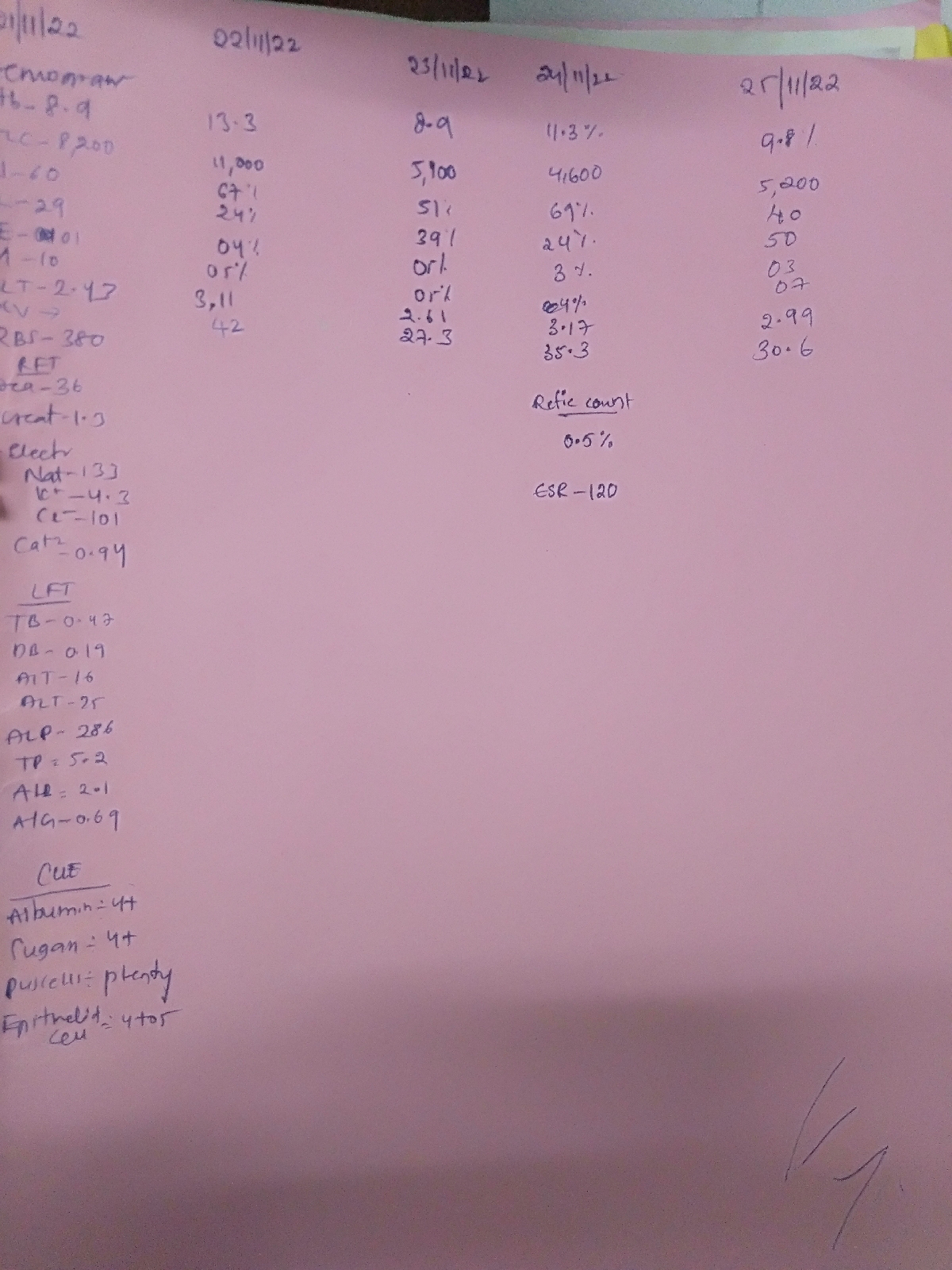
PLEURAL FLUID ANALYSIS
PLEURAL PROTEIN -0.9/SERUM PROTIEN -5.2=0.17
PLEURAL LDH-116/ SREUM LDH-302=0.38
>2/3X460=306
SUGGESTING TRANSUDATIVE FLUID
ACUTE GLOMERULONEPHRITIS WITH ASYMPTOMATIC BACTEURIA
TRANSUDATIVE PLEURAL EFFUSION [SECONDARY TO HYPOALBUMINEMIA?]
RIGHT EYE:TRACTIONAL RETINAL DETACHMENT [B SCAN]
LEFT EYE:SEVERE NPDR CHANGES
WITH K/C/O DM2 [30 YEARS]-HBA1C= 7.5% ON 22/11/22
Treatment Given(Enter only Generic Name)
1.TAB.OFLOXACIN 200MG PO/BD
2.INJ.LASIX 40MG IV/BD
8AM--4PM--X
3.INJ.HAI SUB CUTANEOUS /TID
4U--4U--4U
4.INJ.NPH SUBCUTANEOUS /BD
5U--X--5U
5.PROTEIN-X POWDER IN ONE GLASS OF MILK OR WATER /BD
6. GRBS 7(.) PROFILE MONITIRING
BRIEF COURSE IN HOSPITAL
PT CAME WITH CHIEF C/O PEDAL EEDEMA,FACIAL PUFINESS,FEVER,COUGH.ON CHEST
XRAY IT WAS SHOWING PLEURAL EFFUSION[B/L] FOR WHICH DIAGNOSTIC PLEURAL FLUID
ANALYSIS WAS DONE WHICH SUGSESTING TRANSUDATIVE FLUID.AS SHE IS A KNOWN
CASE OF DIABETES ,FUNDOSCOPY WAS DONE SHOWING
RE:TRACTIONAL RETINAL DETACHMENT ON B SCAN
LE:SEVERE NPDR CHANGES NOTED[TORTUS ,ATTENUATED COTTON WOOLSPOTS+,DOT
HEMORRHAGE SUPERIOR TO DISC+,FIBROUS BANDS EXTENDING FROM DISC].

